While CVR provides immediate results, the procedure is lengthy (3–9 hours), often requires transfusions, and involves longer recovery times.
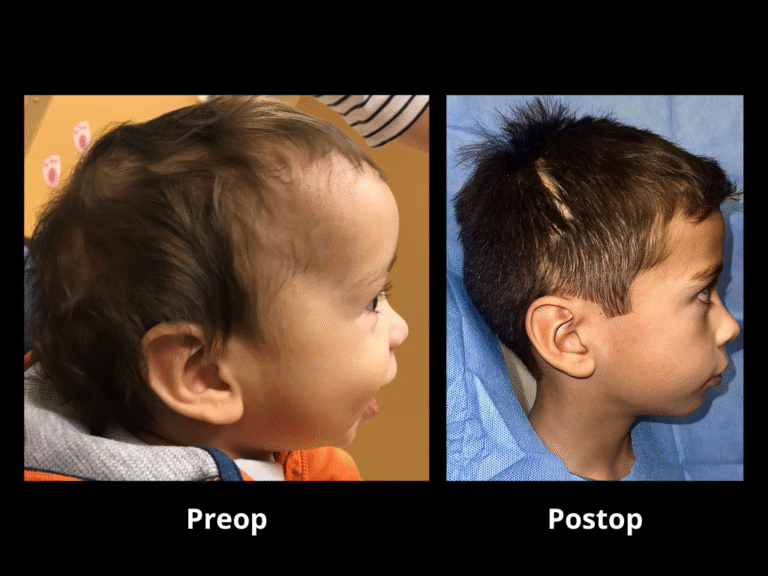
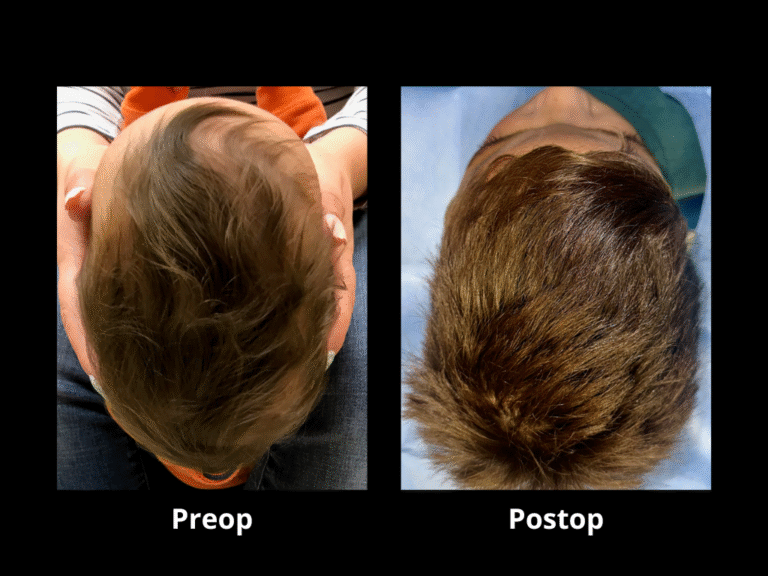
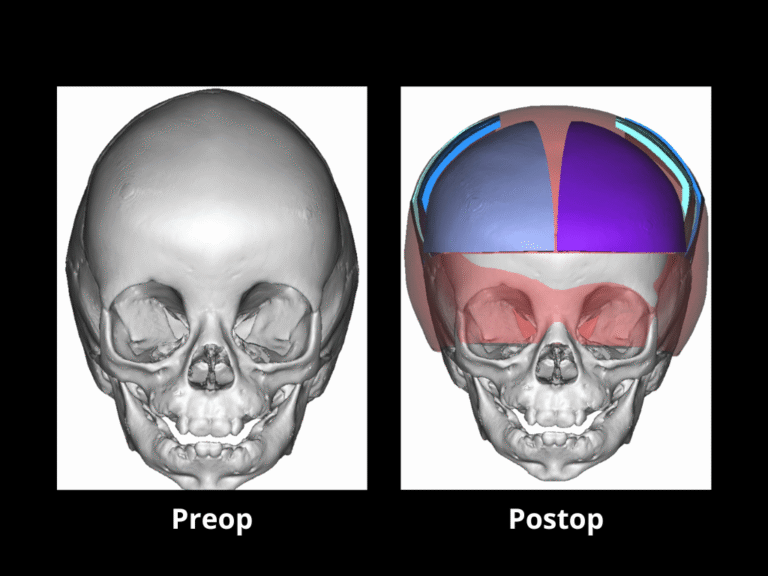
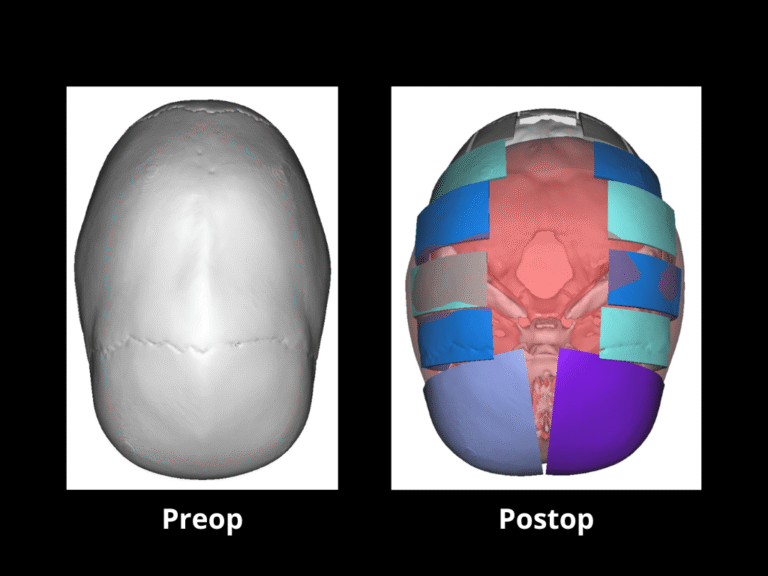
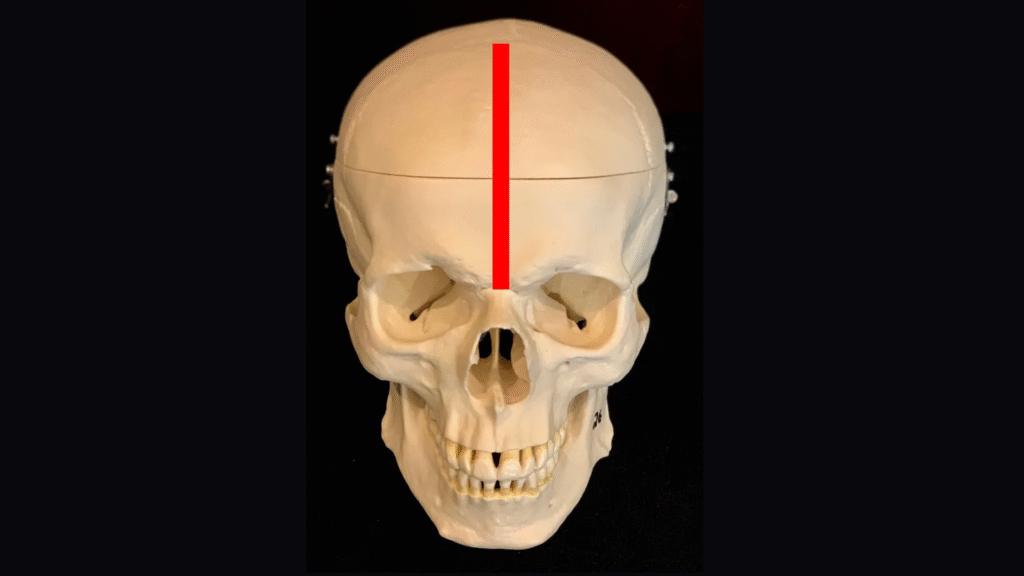
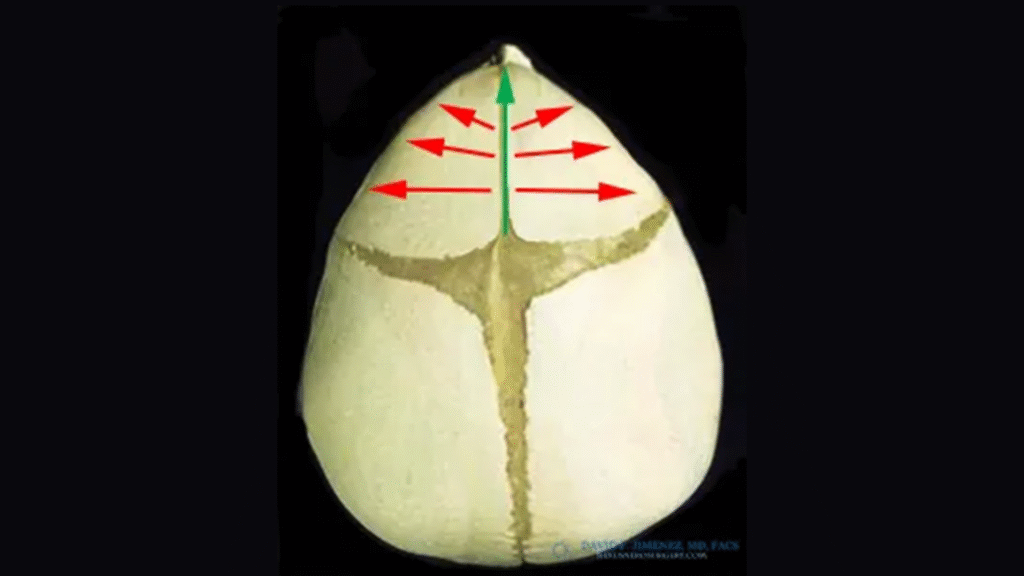
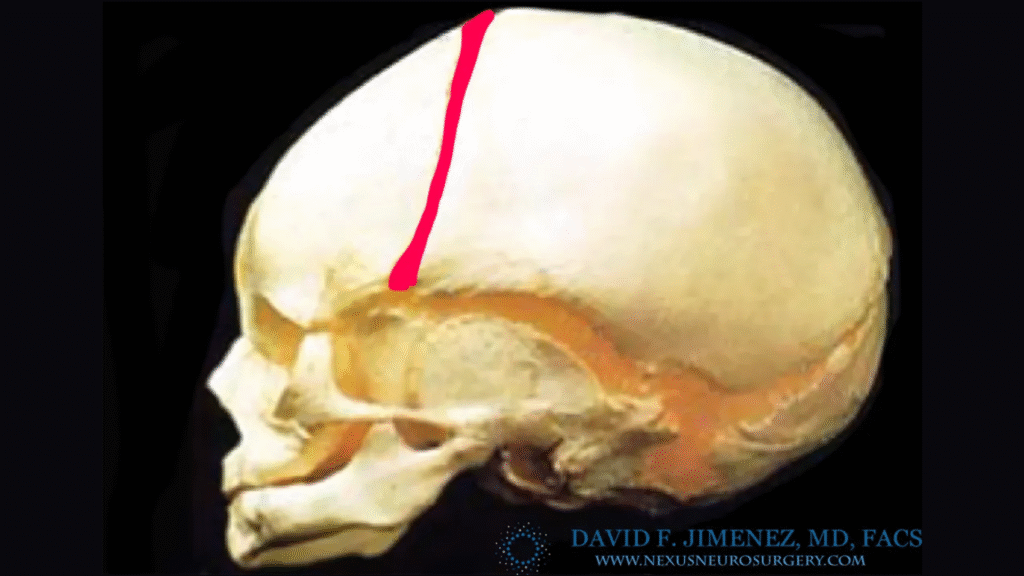
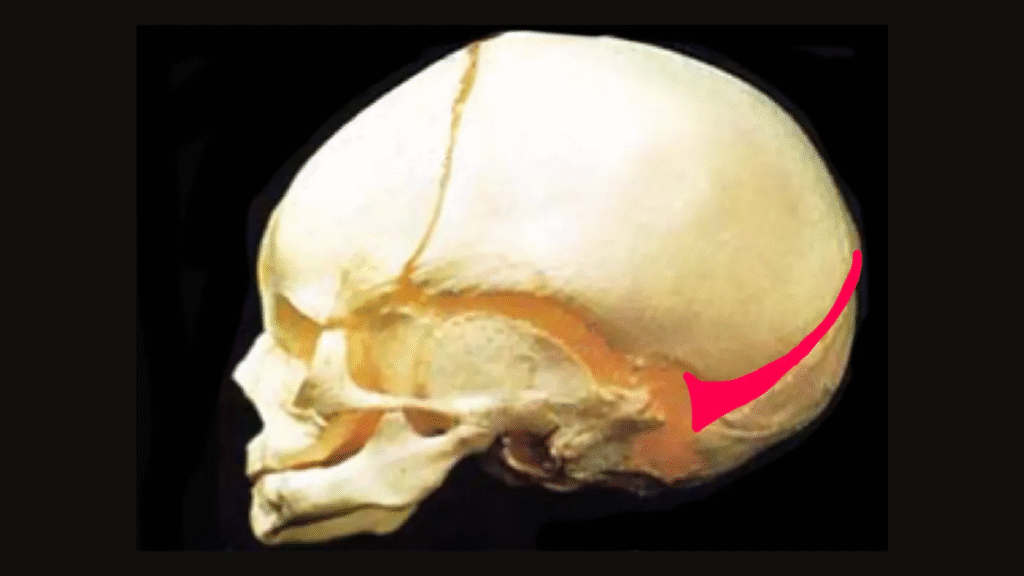
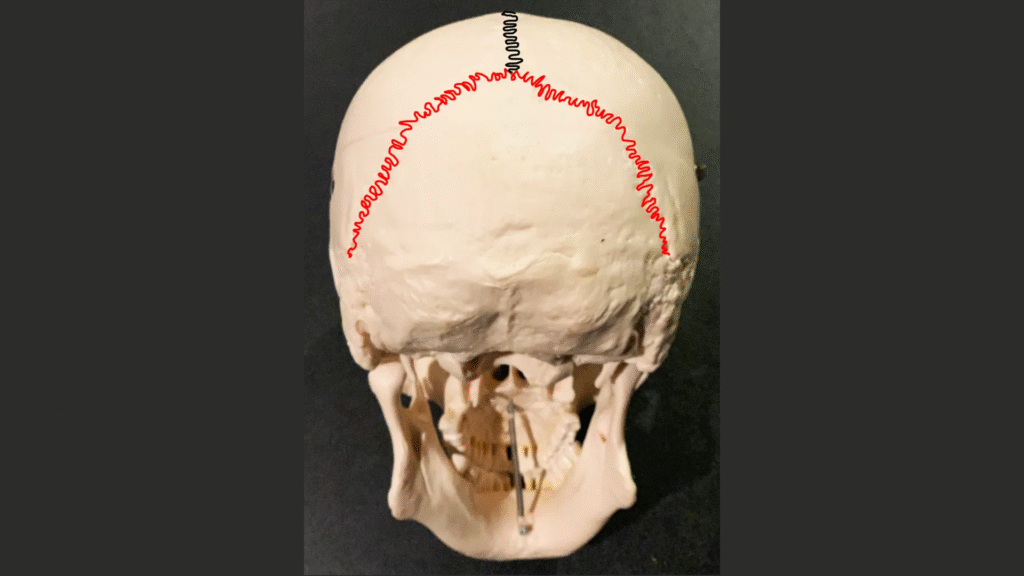
Recognizing these challenges, El Paso Craniofacial Team pioneered the use of endoscopic-assisted surgery more than two decades ago. This minimally invasive technique is performed in very young infants, ideally before 12 weeks of age. Through small incisions, the fused suture is released, allowing the brain’s rapid growth to remodel the skull naturally. Postoperative helmet therapy then helps guide growth into a normal shape.
Custom helmets, manufactured by FDA-cleared Orthomerica Products, Inc., are adjusted regularly to accommodate rapid growth. Helmets do not restrict brain development; instead, they redirect growth safely and effectively.