
Endoscopic-Assisted Surgery
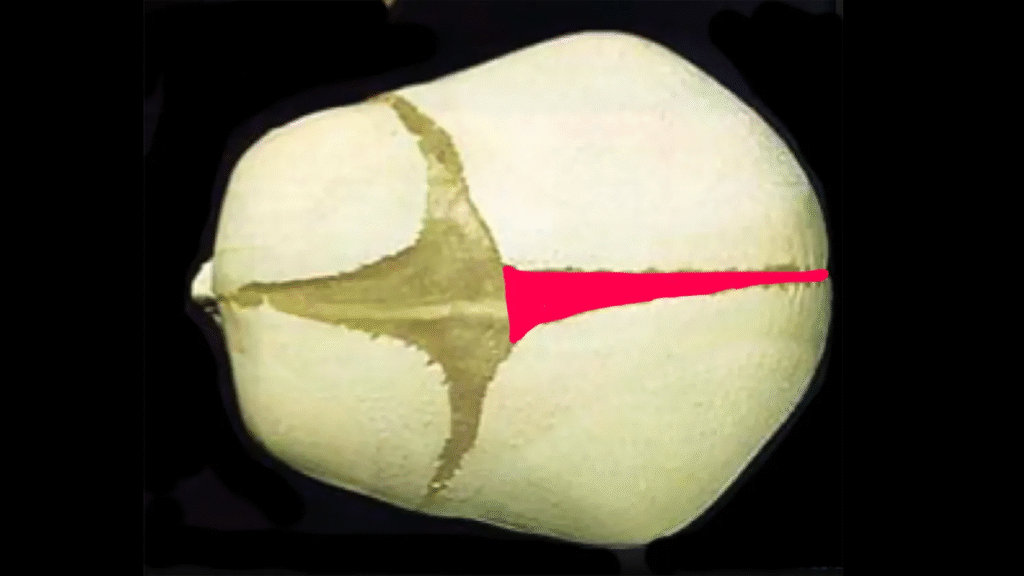
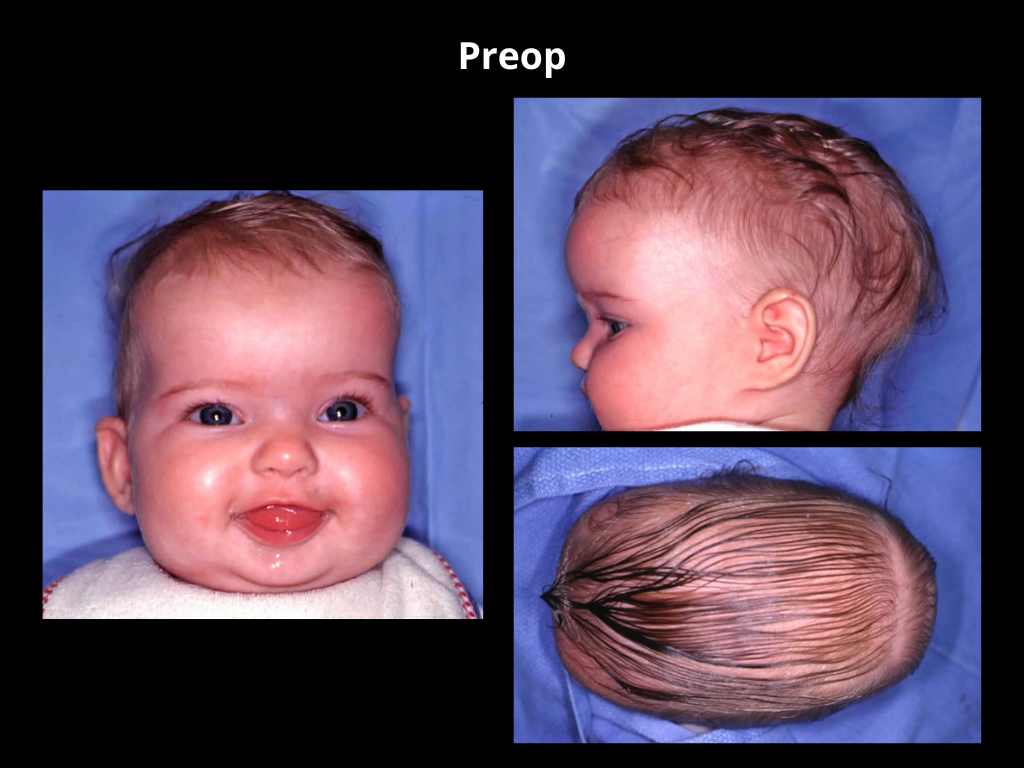
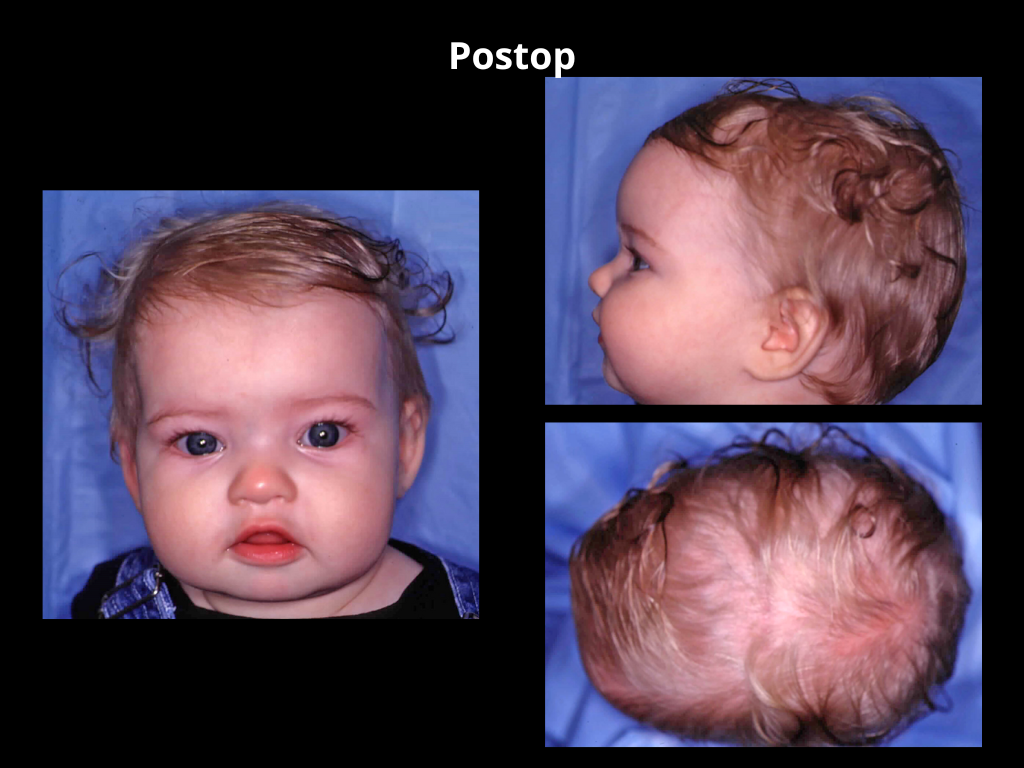
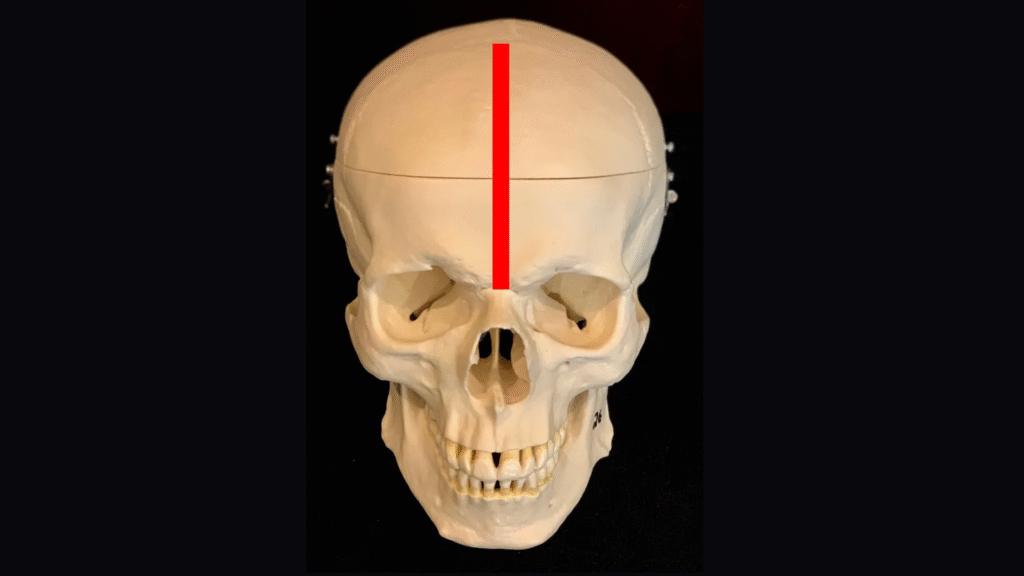
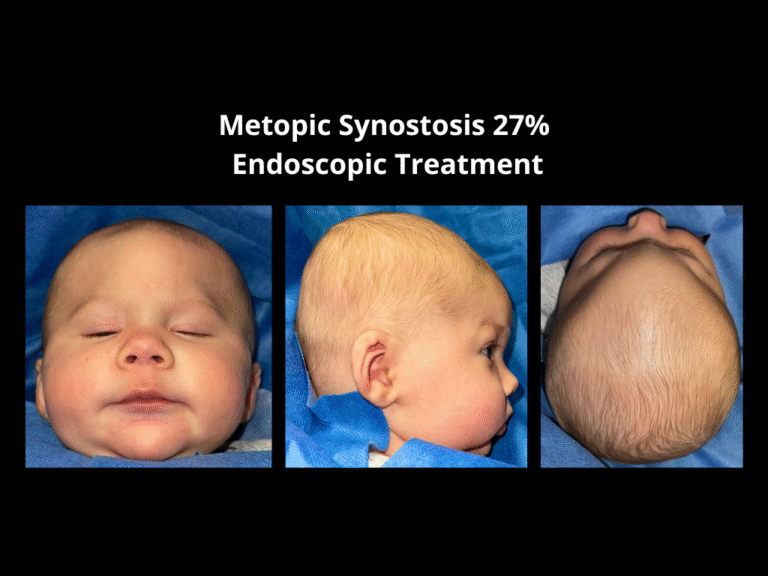
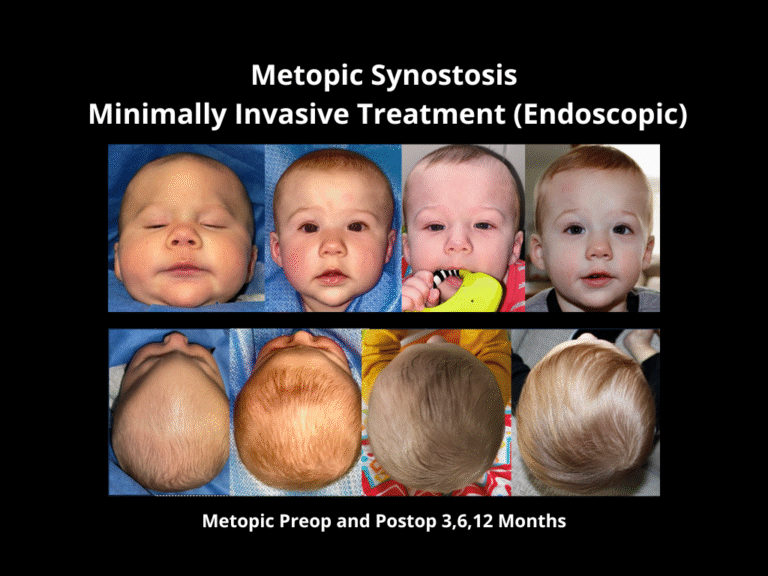
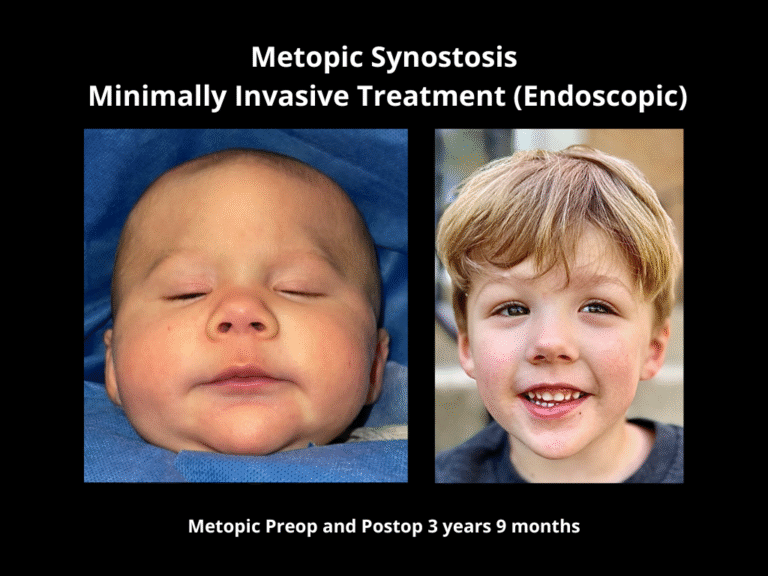
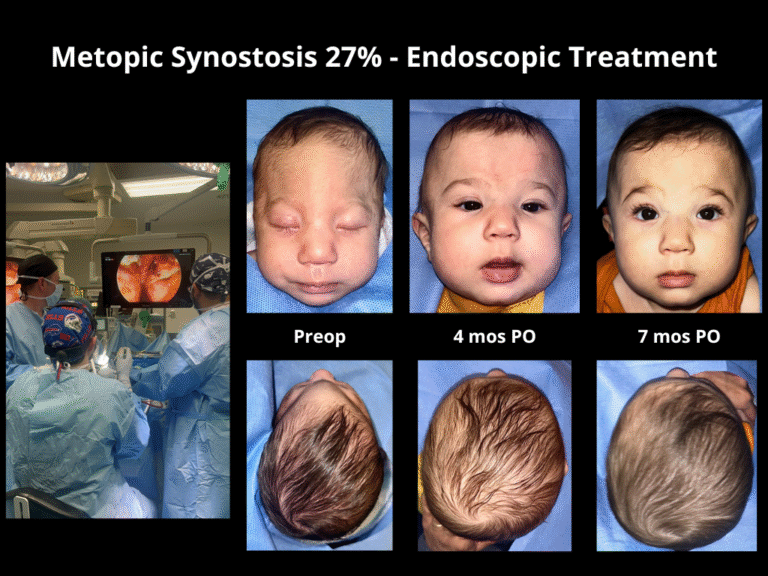
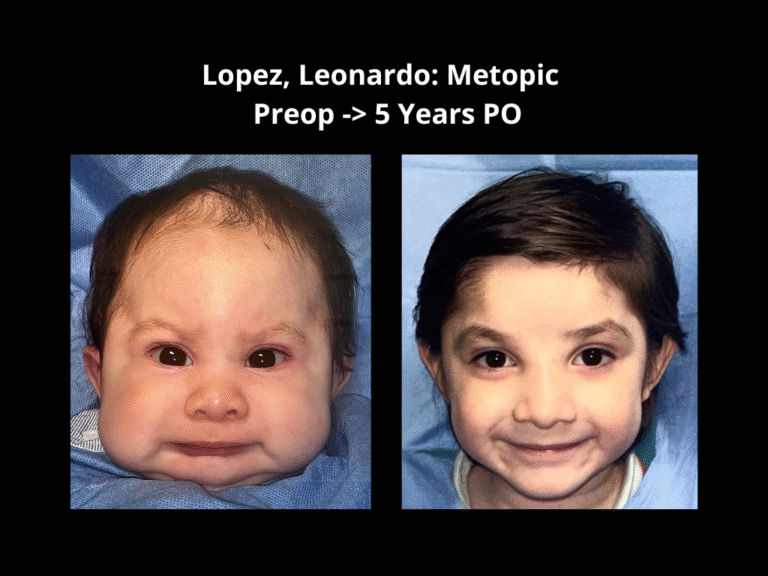
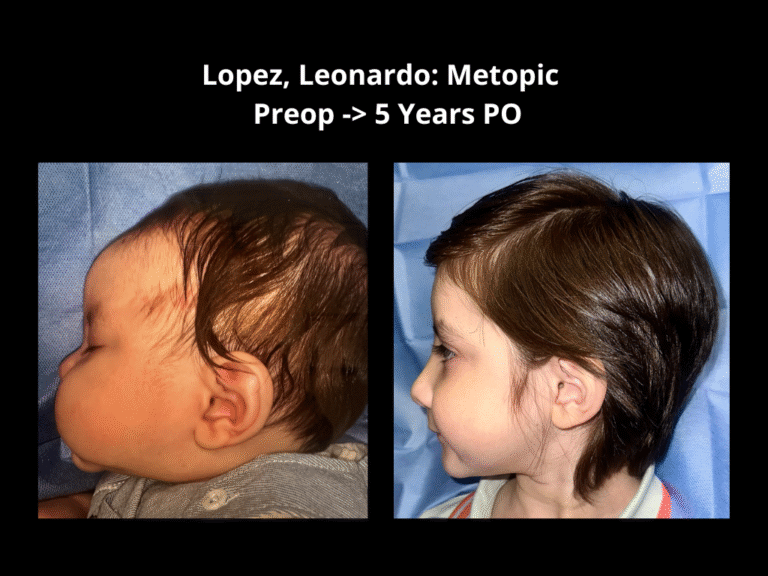
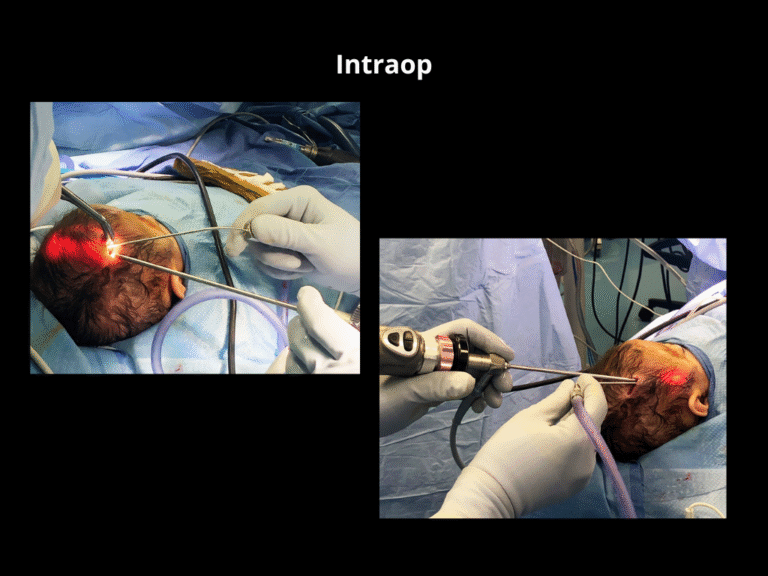
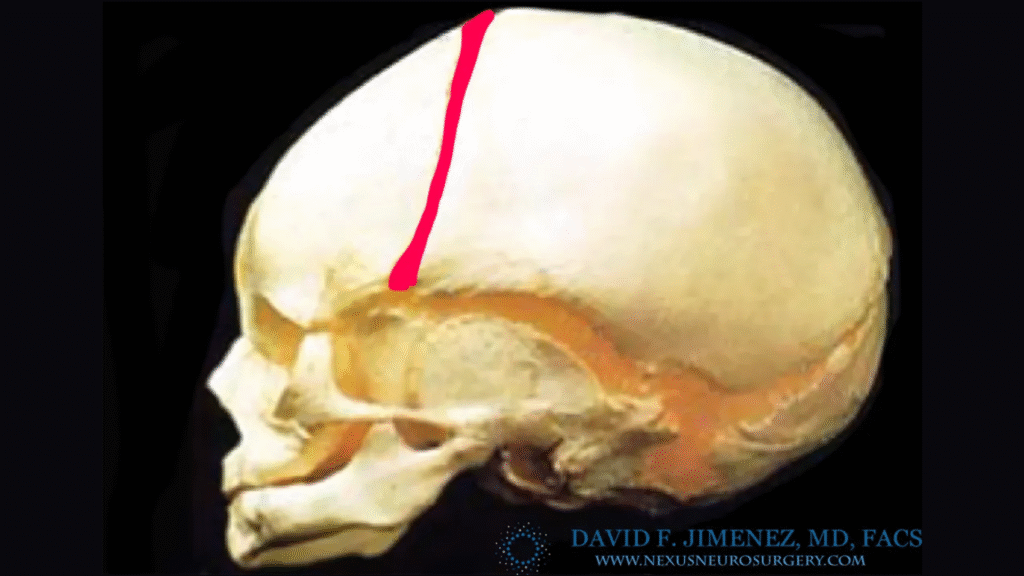
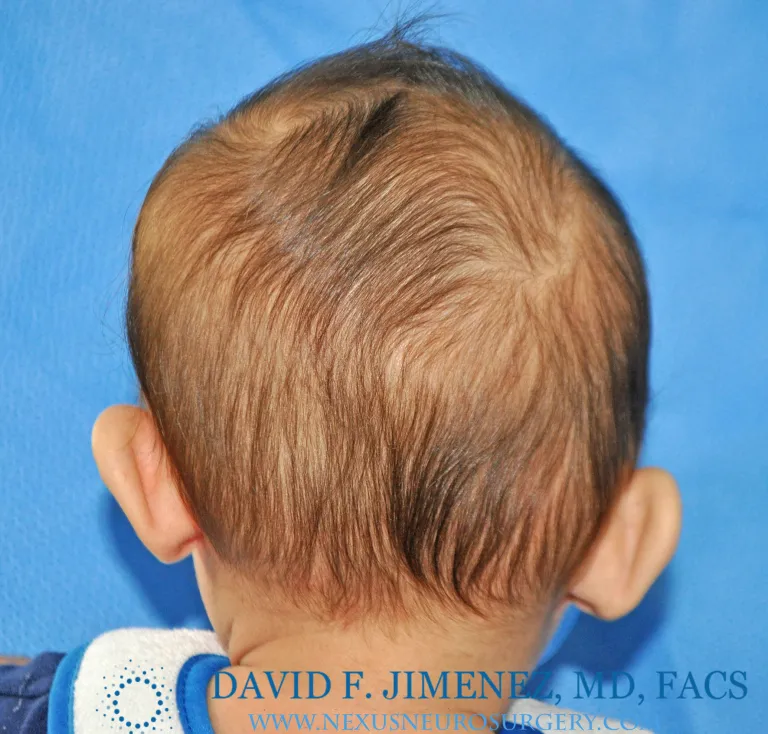
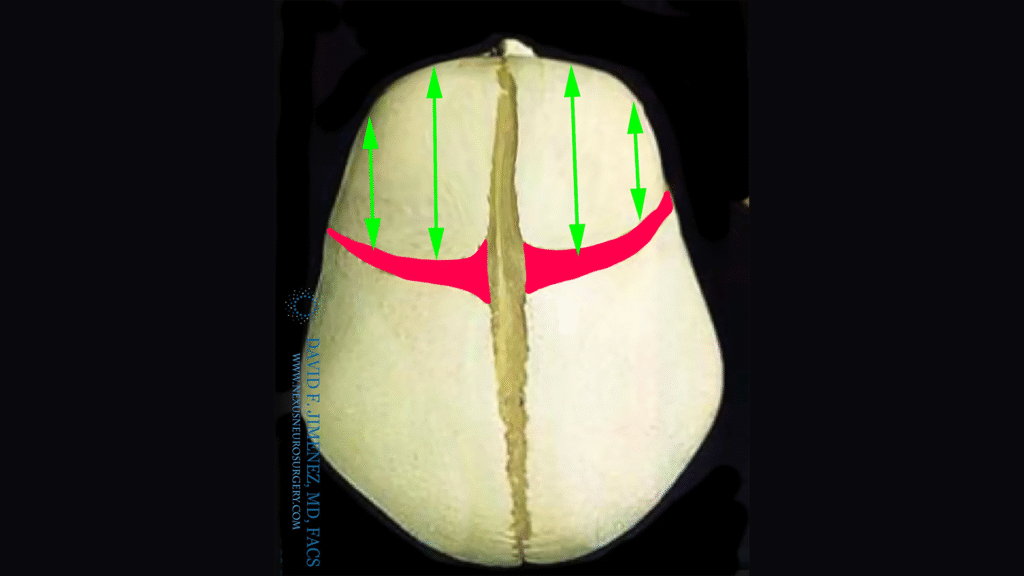
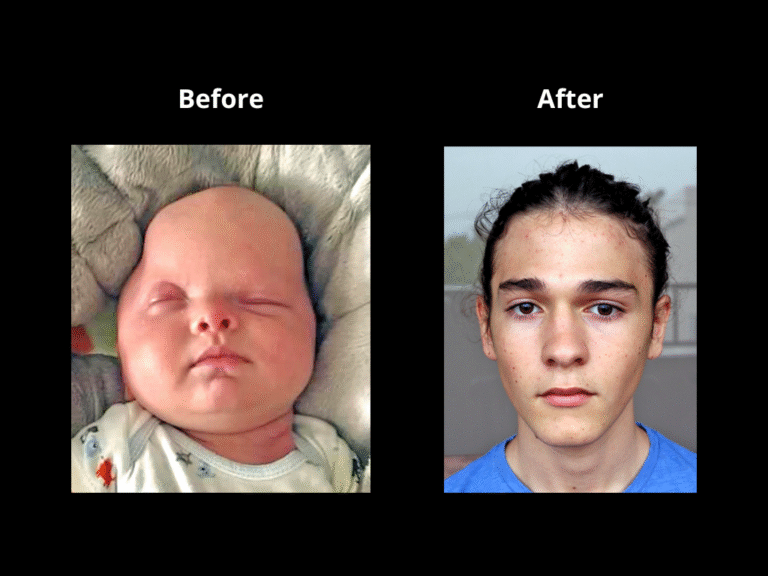
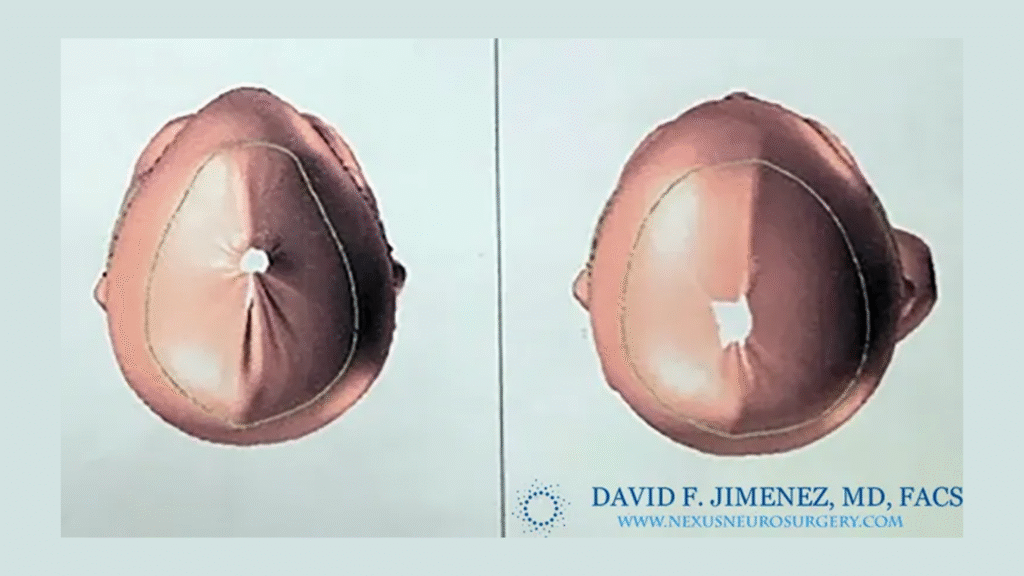
Endoscopic-assisted craniosynostosis surgery is a minimally invasive technique developed to treat infants diagnosed within the first few months of life. Introduced more than two decades ago, this approach allows for safe and early correction of abnormal skull growth by releasing the fused suture through small incisions.
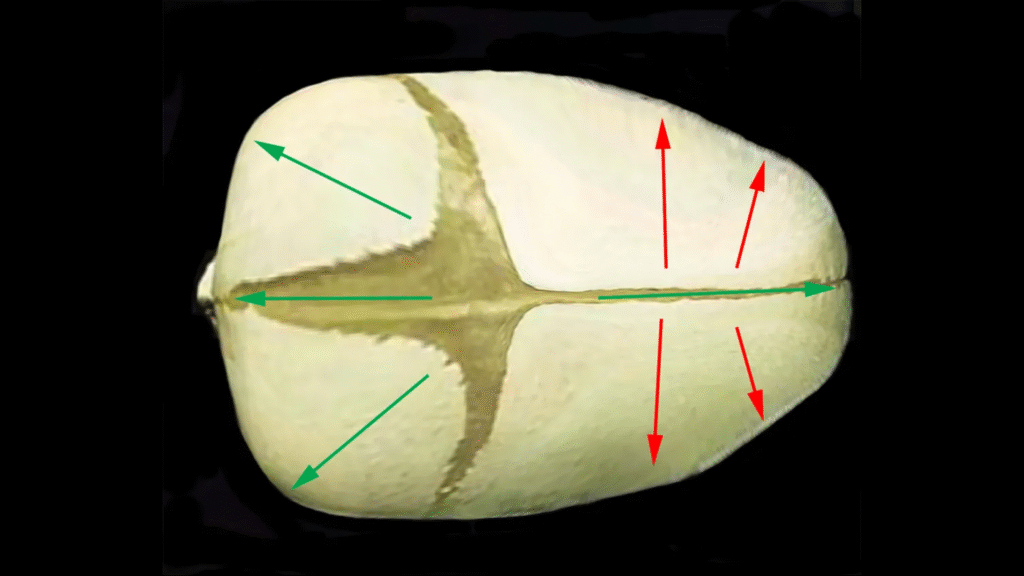
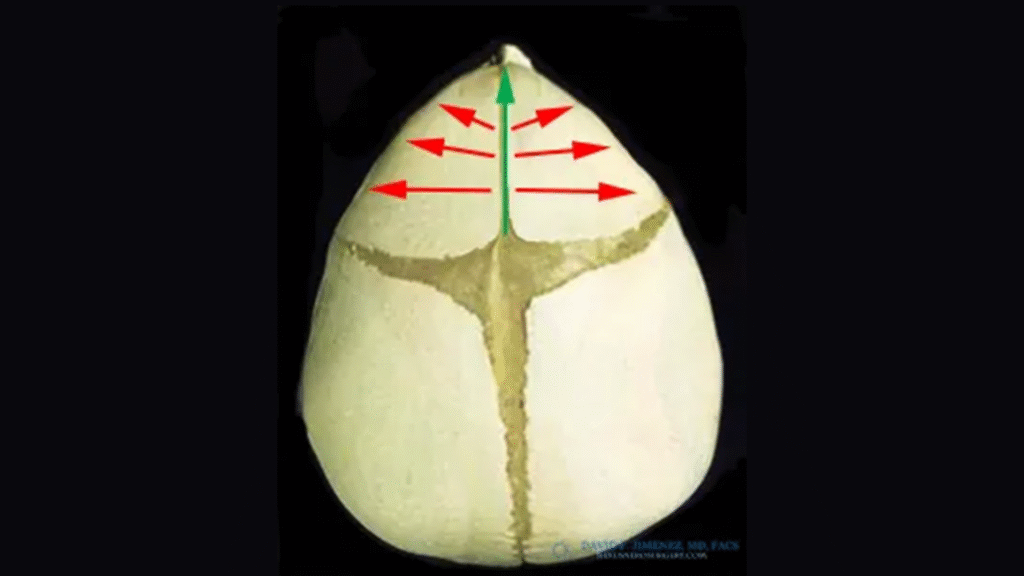
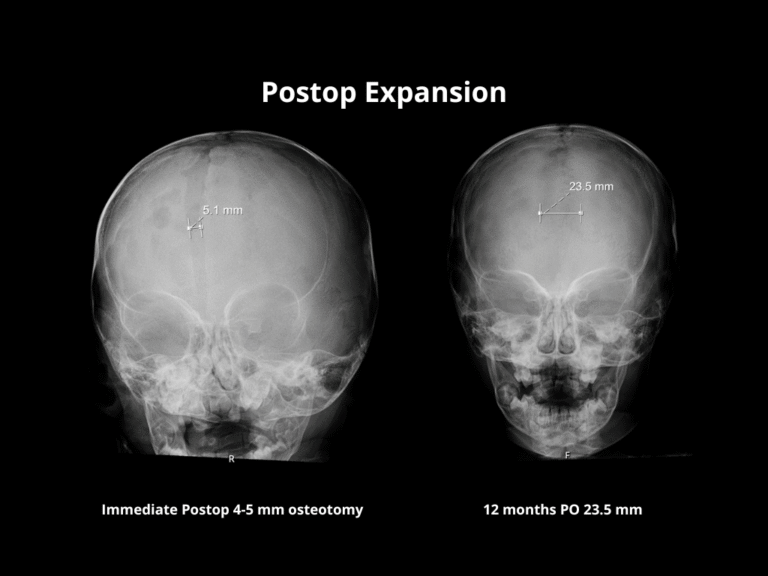
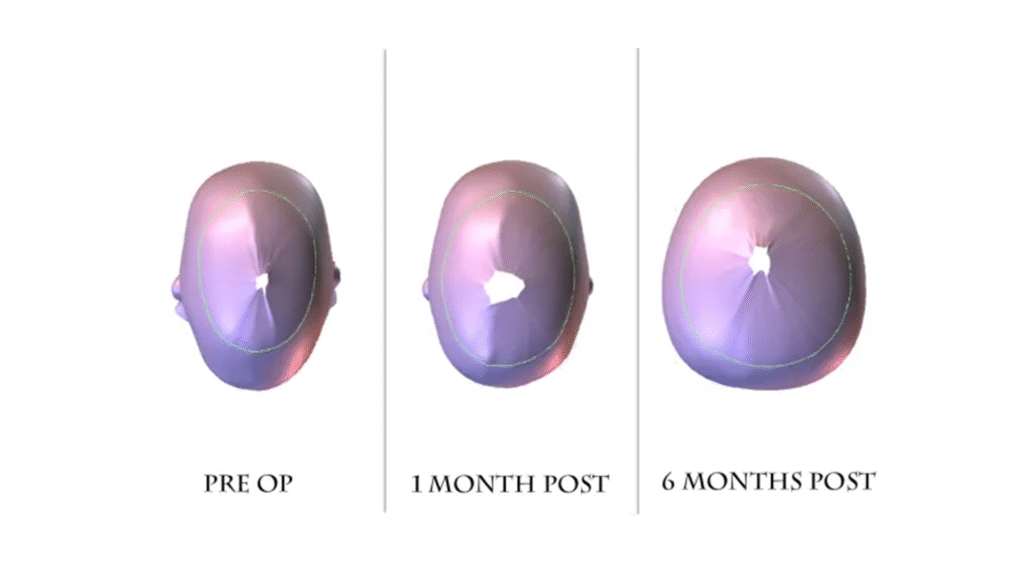
The principle behind the endoscopic method is to use the natural, rapid growth of the infant brain to reshape the skull once the restriction is released. Because the incisions are small and the bone removal limited, this method reduces surgical time, blood loss, swelling, and hospital stay compared to open cranial vault reconstruction.